MBC vs Athenahealth vs R1 RCM are among the most frequently evaluated names when selecting a medical billing company for physician groups, PE-backed specialty networks, and health systems. Each is a fundamentally different medical billing company — built for different clients, operating at different scales, and optimized for different revenue cycle management services outcomes. According to MBC’s 2026 analysis, choosing the wrong one costs practices 2%–8% of collectible revenue annually.
MBC vs Athenahealth vs R1 RCM are among the most frequently evaluated names when physician groups, PE-backed specialty networks, and health systems select a revenue cycle management services partner. There are also three companies with fundamentally different market architectures — built for different clients, operating at different scales, and optimized for different revenue cycle outcomes.
Choosing the wrong medical billing company does not just mean paying for a service that underperforms. It means systematically losing 2%–8% of collectible revenue annually to coding errors, denial mismanagement, and reporting gaps that the wrong vendor is structurally unable to solve — because the problem was never their market to begin with. This is the definition of a practice losing revenue to a structural mismatch, not a billing error.
This comparison evaluates MBC, Athenahealth, and R1 RCM honestly — including where each company is not the right answer — so that CFOs, practice administrators, and physician group owners can make a decision based on their actual organization, not on vendor marketing. It also maps where Medical Billing Services, RCM services, pricing structure, and revenue integrity differ materially across the three.
The One-Line Summary Before the Detail
| Company | Best For | Not Built For |
|---|---|---|
| Medical Billers and Coders (MBC) | Multi-specialty physician groups, PE-backed specialty networks, enterprise specialty practices with $1M+ monthly collections | Hospital systems seeking full patient access outsourcing; solo practitioners seeking all-in-one EHR + billing |
| Athenahealth | Large health systems and hospital networks already invested in the athenaOne platform, seeking unified EHR + billing technology. | Independent specialty practices requiring subspecialty coding depth; mid-market groups needing dedicated account management |
| R1 RCM | Hospital systems and large health networks require fully outsourced enterprise-scale revenue cycle operations | Independent physician groups; specialty practices; mid-market multi-specialty organizations under $50M in annual revenue |
Head-to-Head Comparison: MBC vs Athenahealth vs R1 RCM
| Evaluation Criterion | MBC | Athenahealth | R1 RCM |
|---|---|---|---|
| Market Architecture | Specialty-focused RCM company | Cloud-based EHR + billing technology platform | Enterprise hospital RCM outsourcing company |
| Specialty Coding Depth | Subspecialty-certified coders across 40+ specialties | Technology-driven generalist coding | Hospital-focused, generalist for specialty practices |
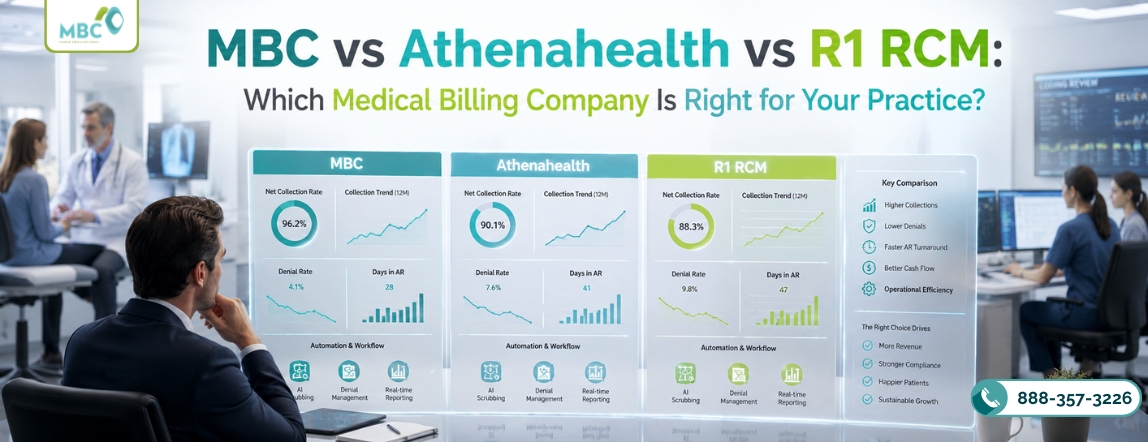
| Net Collection Rate | 97%+ for specialty groups | ~93% FPAR reported (NCR varies by client) | Varies; optimized for hospital NCR metrics |
| Denial Management | Root-cause analytics, specialty-specific denial protocols | Payer rule engine automation | Enterprise denial management infrastructure |
| EHR Integration | EHR-agnostic — works with any system | Requires the AthenaOne platform; limited external EHR integration | Multi-system integration for hospital environments |
| Account Management | Dedicated specialty account managers | Technology-first; limited human account management for mid-market clients | Enterprise relationship management for health system clients |
| Reporting | CFO-grade specialty dashboards: NCR, Days in AR, payer variance, denial root-cause | AthenaOne platform reporting suite | Enterprise health system financial reporting |
| Pricing Model | 4%–8% of net collections, specialty-dependent | 4%–7% of collections (platform + billing combined) | Percentage of net patient revenue; enterprise pricing |
| Minimum Scale | Multi-provider specialty groups | Mid-to-large health systems | Health systems; $50M+ annual revenue |
| Best Fit | Specialty practices, PE-backed networks, enterprise multi-specialty groups | Hospital networks on the athenaOne platform | Hospital systems, academic medical centers, and large health networks |
Medical Billers and Coders (MBC): Detailed Assessment
Medical Billers and Coders is built around a premise that neither Athenahealth nor R1 RCM operates from: that specialty-specific coding expertise — not technology automation or enterprise scale — is the primary driver of Net Collection Rate performance for physician groups and specialty networks. As a specialty-experienced RCM partner, MBC’s entire operational architecture is designed to meet the Medical Billing Services requirements of multi-specialty groups, not hospital systems or solo practitioners.

Where MBC Wins
- Subspecialty Coding Accuracy at Scale: MBC deploys certified coders with subspecialty-specific training across 40+ specialties — including orthopedic, wound care, ASC, dermatology, OB-GYN, and optometry. This is not cross-trained generalist knowledge — it is dedicated subspecialty expertise that produces 97%+ NCR outcomes by eliminating the specialty-specific coding errors that drive denial volume in complex procedure mixes. How medical billers and coders help physicians sustain this NCR level is through dedicated subspecialty coders who know each specialty’s modifier rules, payer-specific payment policies, and denial patterns by procedure category — not through a generalist coding pool that applies national billing rules uniformly.
- EHR-Agnostic Operations: MBC integrates with any EHR or practice management system without requiring a platform migration. This is critical for specialty practices that have already invested in an EHR system and do not want the selection of a medical billing company to dictate technology choices. It also preserves the independent audit layer — the separate review of clinical documentation against billing claims — that integrated EHR + billing systems eliminate. When the same vendor controls both documentation and billing, the independent revenue integrity detection mechanism disappears. Separating EHR from billing is the structural foundation of revenue integrity for specialty practices.
- CFO-Grade Specialty Reporting: MBC provides facility-specific NCR trending, payer variance analysis, denial root-cause analytics by procedure category, and Days in AR reporting by physician and location — the financial visibility that multi-site administrators and PE-backed group CFOs require to make staffing, contracting, and capacity decisions in the context of revenue cycle management services.
- Old AR Recovery: MBC’s Old AR Recovery capability addresses the revenue that practices have already lost to aged AR write-off drift — claims in the 12–24 month prior period that were never appealed, never followed up, and have been mentally written off. Old AR Recovery is a standard component of MBC’s initial engagement, not an add-on service. For practices switching from a prior medical billing company that did not systematically manage aged AR, the Old AR Recovery component typically returns $40,000–$120,000 in the first 90 days.
- 25 Years of Documented Enterprise RCM: MBC’s 25+ year operating history across hospital systems, PE-backed multi-site groups, and enterprise specialty networks provides a track record of NCR performance and compliance infrastructure that newer technology-first competitors cannot match with platform metrics alone.
Where MBC Is Not the Right Fit
MBC is not built for solo practitioners seeking an all-in-one EHR and billing solution. It is not optimized for hospital systems that require full patient-access outsourcing — including front-desk scheduling, registration, and pre-authorization infrastructure at hospital scale. Organizations with these requirements should evaluate Athenahealth or R1 RCM, respectively.
Athenahealth: Detailed Assessment
Athenahealth is one of the most recognized names in healthcare technology, and its athenaOne platform — combining EHR, practice management, and billing — delivers genuine value for large health systems that have built their clinical and administrative operations around it. Its payer rule engine processes connections across thousands of payers and achieves a documented 93% first-pass acceptance rate for claim submissions.
Where Athenahealth Wins
For health systems already embedded in athenaOne, Athenahealth’s unified platform reduces the administrative friction between clinical documentation, scheduling, and billing claim generation. Its network effects — payer rule updates propagated across its entire client base — provide a meaningful defense against claim-scrubbing failures driven by payer policy changes.
Athenahealth’s patient engagement tools and scheduling infrastructure add clinical operations value that a standalone medical billing company cannot provide — making it genuinely differentiated for organizations that want a single vendor managing clinical and revenue cycle management services technology simultaneously.
Where Athenahealth Falls Short for Specialty Groups
Technology-First, Service-Second Athenahealth’s model prioritizes platform automation over dedicated account management. Multi-specialty groups with complex payer negotiations and high-acuity procedure coding requirements frequently report that resolving complex billing issues requires slow, generalist escalation paths — because the model is built to automate, not to manually intervene with subspecialty expertise. A specialty-experienced RCM partner with dedicated account management is structurally different from a technology platform with a billing module.
Generalist Coding for Complex Specialties Athenahealth’s billing strength is its payer rule engine — not subspecialty coding depth. Independent orthopedic groups, wound care centers, ASCs, and other procedurally complex specialties consistently report gaps in coding accuracy for high-acuity subspecialty procedures compared with a dedicated specialty medical billing company.
Platform Lock-In Athenahealth’s billing capabilities are maximized within athenaOne. Organizations not already on the platform face significant migration investment to access the billing services, and organizations on the platform face significant switching costs to leave. This lock-in dynamic is a strategic consideration for PE-backed groups that may need to integrate billing infrastructure across acquired practices on multiple EHR systems.
R1 RCM: Detailed Assessment
R1 RCM is purpose-built for hospital-scale revenue cycle outsourcing. It manages end-to-end RCM services — including patient access, charge capture, coding, claim submission, denial management, and financial reporting — for some of the largest health systems in the United States. Its operational infrastructure is designed for the claim volume, organizational complexity, and regulatory compliance requirements of multi-facility hospital networks.
Where R1 RCM Wins
For hospital systems seeking to fully outsource their revenue cycle operation — transferring staff, technology, and management accountability to a single enterprise partner — R1 RCM offers infrastructure depth and operational scale that specialty-focused billing companies cannot match. Its enterprise relationship model, dedicated implementation teams, and health system-specific compliance controls are genuinely differentiated for the hospital market.
Where R1 RCM Is Not the Right Fit
R1 RCM’s operational architecture is not calibrated for independent physician group billing. Its pricing structure, minimum scale requirements, and service delivery model are designed for health systems with tens of millions in annual net patient revenue — not for specialty practices with $1M–$10M in annual collections. Specialty practices evaluated by R1 RCM as a potential client are often directed to a different tier of service that does not include the enterprise infrastructure that defines R1’s market reputation.
Additionally, R1’s hospital-focused coding infrastructure does not deliver the subspecialty depth that procedurally complex orthopedic, wound care, or ASC practices require. Hospital coders are trained in a broad range of diagnosis-related groups (DRGs) and inpatient coding, not in the modifier-intensive, measurement-based, globally tracked procedure coding that defines specialty practice billing — and that a specialty-experienced RCM partner must master.
The EHR-Agnostic Advantage: Why It Matters for the Comparison
Athenahealth requires platform adoption. R1 RCM works with health system technology stacks. MBC is EHR-agnostic.
For PE-backed physician groups acquiring practices across multiple EHR systems, the EHR-agnostic model is not a convenience — it is a structural requirement. A medical billing company that requires platform migration as a condition of service creates acquisition friction, technology transition cost, and a period of billing disruption that destroys the NCR improvement the acquisition was supposed to generate.
Beyond acquisition scenarios, the EHR-agnostic model preserves the independent audit layer. When the same vendor manages both clinical documentation and billing claim generation, coding errors embedded in documentation templates are replicated into billing claims without independent review. Separating EHR from billing creates an independent checkpoint that catches errors produced by the integrated system — a structural revenue-integrity mechanism that integrated platforms cannot provide for themselves. This is the single most important structural difference between MBC and both Athenahealth and R1 RCM from a revenue integrity standpoint.
Revenue Diagnostic: How to Know Which Company Is Right Before You Sign
Before selecting any medical billing company, a revenue diagnostic benchmarks where your practice currently sits — NCR, denial rate by specialty, AR aging distribution, payer underpayment variance — and quantifies the specific revenue recovery opportunity available. Without a revenue diagnostic, the selection decision is based on vendor marketing rather than the actual dollar gap between where your practice is and where it should be.
MBC’s revenue diagnostic is delivered in 30 days and includes: NCR trending by specialty and payer, denial root-cause analysis, Days in AR by physician and location, Old AR Recovery opportunity quantification, and a benchmark comparison against the CMS and MGMA performance standards for your specialty. The output is a dollar-quantified revenue gap — not a sales pitch.
FAQs: MBC vs Athenahealth vs R1 RCM
The fundamental difference is market architecture. MBC is a specialty-focused RCM company designed for multi-specialty physician groups and enterprise specialty networks requiring subspecialty coding depth. Athenahealth is a cloud-based technology company that combines EHR and billing, optimized for large health systems, embedded in its athenaOne ecosystem. R1 RCM is an enterprise outsourcing company purpose-built for hospital systems requiring fully outsourced revenue cycle operations. Each is the right answer for a different type of organization — and the wrong answer for the other two.
Athenahealth is optimized for large health systems and hospital networks already integrated into athenaOne. For independent specialty practices — orthopedic groups, wound care centers, ASCs, dermatology practices — Athenahealth’s generalist coding model and technology-first service delivery create performance gaps in subspecialty coding accuracy, specialty denial management, and dedicated account management for complex reimbursement issues.
R1 RCM is one of the largest enterprise revenue cycle outsourcing companies in the U.S., purpose-built for hospital systems requiring end-to-end RCM outsourcing at a hospital-network scale. For independent physician groups, specialty practices, and multi-specialty organizations with under $50M in annual revenue, R1 RCM is over-engineered and under-specialized for the subspecialty coding requirements that drive NCR performance in these settings.
MBC’s pricing is structured as 4%–8% of net collections, depending on specialty complexity. Athenahealth ranges from 4%–7% for the combined platform and billing module. R1 RCM pricing for hospital-scale outsourcing is structured as a percentage of net patient revenue at enterprise scale. The relevant ROI question is not per-percentage-point cost — it is which company produces the highest NCR, because a 1% NCR improvement on $5M in collections equals $50,000 in additional annual revenue, regardless of whether the vendor is billing at 5% or 7%.
Ask four questions: (1) Is your practice an independent specialty group, health system-affiliated network, or hospital system? The answer determines which vendor is even relevant. (2) What NCR has each vendor documented for practices of your specialty and scale? (3) Does your practice require EHR and billing from the same vendor, or can you operate EHR-agnostically? (4) What is your annual collections volume, and does the vendor’s operational model match your scale?

A Subject Matter Expert in healthcare billing operations with nearly 10 years of experience, sharing insights on claims processing, coding support, and revenue cycle optimization. Dedicated to educating healthcare professionals on compliance, accuracy, and strategies to improve billing performance.





